


In the scorching heat of midsummer, when most people in the West seek relief in air‑conditioned rooms and iced beverages, a remarkable traditional medical practice draws millions of patients to hospitals and clinics across China. This therapy, known as the dog‑day patch or summer plaster treatment, is one of the most vivid applications of the ancient principle of "treating winter ailments during the summer season" – a concept that may appear paradoxical to those unfamiliar with East Asian medical traditions, yet has been refined through more than two millennia of clinical observation and systematic documentation.

The practice is timed to the three ten‑day periods that constitute the hottest part of the Chinese solar calendar, roughly corresponding to the "dog days" of July and August in the Northern Hemisphere. According to classical medical theory, these are the days when the body’s vital warmth – the active, metabolic energy that sustains life – reaches its annual peak, mirroring the flourishing growth of nature. It is precisely during this window of maximum external heat that the patch therapy is administered, based on the belief that the body’s surface channels are most open, its defensive energy is most vigorous, and its internal organs are most receptive to external medicinal stimulation.

The philosophical roots of this treatment lie in the Yellow Emperor’s Classic of Internal Medicine, a foundational text compiled over two thousand years ago, which articulates the principle of nourishing the active principle in spring and summer. In this framework, many ailments that flare up or become debilitating during cold weather – such as bronchial asthma, chronic bronchitis, allergic rhinitis, recurrent respiratory infections, and arthritic joint pain aggravated by chill – are understood to stem from a constitutional deficiency of internal warmth and an accumulation of cold, damp pathogens deep within the body. These are collectively referred to as "winter diseases." By intervening at the height of summer, when the external environment supplies abundant thermal energy, practitioners aim to replenish the body’s internal warmth, expel the stored cold, and reinforce the immune barriers before the next winter arrives.
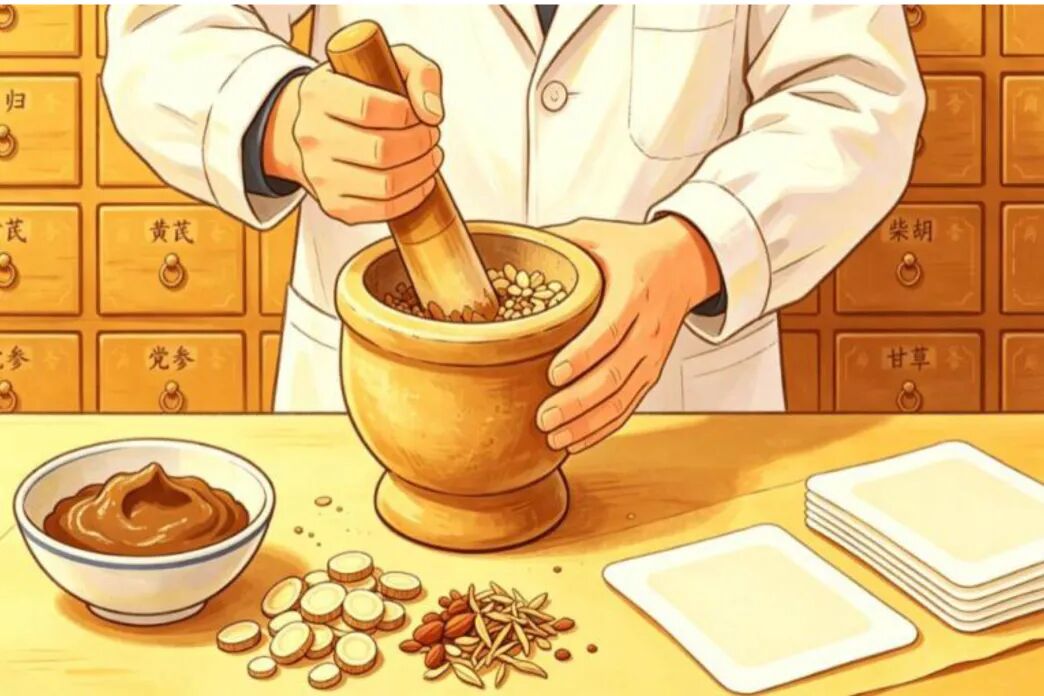
The modern plaster formulation traces its documented history to the Ming dynasty, with a more detailed recipe appearing in the Qing‑era medical compendium of the physician Zhang Lu. The classic mixture consists of ground white mustard seeds, corydalis tuber, kansui root, and wild ginger – all pungent, warming herbs – blended with fresh ginger juice to form a thick paste. This paste is spread onto small adhesive pads and applied to selected acupoints, most commonly on the upper back, along the urinary bladder meridian. The original version was intentionally designed to produce mild blistering and local redness, a reaction thought to intensify the therapeutic effect; hence it was sometimes called "heavenly blistering." Contemporary formulations have been modified to reduce blistering while preserving the strong cutaneous stimulation, making the treatment more acceptable to modern patients while retaining its fundamental mechanism.
The selection of acupoints follows a rationale deeply rooted in meridian theory. The points most frequently chosen include those located at the seventh cervical vertebra, between the shoulder blades, and on either side of the thoracic spine – areas where the bladder meridian and the governing vessel converge. These sites are considered the "sea of the active channels" because they receive and distribute warming energy to the lungs, spleen, and kidneys. When the herbal plasters are applied, the pungent and heat‑producing ingredients penetrate the skin and travel along the meridian pathways, reaching the internal organs that are most vulnerable to cold invasion. The local inflammation and increased blood flow further stimulate the body’s own repair and regulatory systems, creating a lasting conditioning effect that extends well beyond the summer months.

From a physiological perspective, the patch therapy operates on several complementary levels. First, the active compounds in the mustard seeds and ginger – including sinigrin and gingerol – induce a mild, controlled inflammatory response that recruits immune cells to the skin, thereby modulating systemic immune activity. Second, the sustained local heat and irritation trigger the release of endogenous opioids and anti‑inflammatory cytokines, which may reduce airway hyper‑reactivity and joint pain in susceptible individuals. Third, the repeated stimulation of specific cutaneous zones is believed to rebalance autonomic nervous function, improving bronchial tone and digestive motility. Clinical studies conducted in Chinese tertiary hospitals have shown that patients with moderate‑to‑severe allergic rhinitis who undergo a full three‑year course of summer patches experience a significant reduction in symptom frequency and medication use, with some trials reporting improvement rates exceeding 50 percent.
The treatment is not prescribed indiscriminately; it is indicated primarily for a well‑defined set of chronic conditions. In respiratory medicine, it is recommended for asthmatic patients, especially those whose attacks are triggered by cold air or seasonal changes, as well as for individuals with chronic obstructive pulmonary disease, persistent cough, and recurrent childhood respiratory infections. In gastroenterology, it is used for those suffering from cold‑type stomach pain, chronic diarrhoea, and poor digestion that worsens in winter. In orthopaedics, it is applied to cervical spondylosis, frozen shoulder, and osteoarthritis – particularly when these are accompanied by a subjective feeling of cold and stiffness in the affected joints. In gynaecology, women with painful menstruation and irregular cycles related to cold constitution may also benefit. The therapy is also increasingly sought by younger adults experiencing sub‑health states, such as persistent fatigue, cold intolerance, and frequent minor illnesses, as a form of preventive immunomodulation.

The administration schedule adheres strictly to the dog‑day calendar. Traditionally, the plasters are applied on the first day of each of the three ten‑day periods. In contemporary practice, however, it has become acceptable to receive the treatment on any convenient day within each window, provided that an interval of seven to ten days is maintained between successive applications. A standard course comprises three sessions per summer; many clinicians recommend an additional "reinforcing" session at the end of the final period for patients with severe or long‑standing conditions. For optimal and sustained benefit, a consecutive three‑summer protocol is strongly advised, as the cumulative effect is considered far more meaningful than a single season’s treatment. The wearing time varies: adults typically retain the patches for four to six hours, while children and individuals with delicate skin are advised to remove them after one to two hours to avoid excessive blistering.
Despite its widespread acceptance, the patch therapy carries important precautions and exclusions. It is strictly contraindicated during pregnancy, because the potent warming and blood‑circulating herbs may affect uterine stability. Children under two years of age are generally not treated, owing to their immature skin and higher risk of adverse reactions. Patients with acute febrile illnesses, active infections, or uncontrolled systemic diseases should postpone the procedure until their condition stabilises. Those with skin lesions, ulcers, or dermatological infections at the intended application sites, as well as individuals with known allergies to any of the herbal ingredients or with keloid‑prone skin, are advised against this therapy. Furthermore, persons with internal heat syndromes – characterised by dry mouth, night sweats, and a sensation of heat in the palms and soles – are considered unsuitable, as the warming treatment would exacerbate their underlying imbalance rather than correct it.

Patients undergoing the treatment are given a set of behavioural guidelines to maximise its efficacy. On the day of application, they are instructed to avoid cold drinks, raw fruits, spicy foods, and seafood, which are thought to interfere with the medicinal action. Exposure to air‑conditioning draughts, cold showers, swimming, and prolonged contact with cold surfaces should be minimised for at least twenty‑four hours after the plaster is removed. Mild redness, warmth, and a tolerable itching sensation at the patch sites are normal and desirable signs of effective stimulation. However, if severe burning pain, extensive blistering, or spreading erythema occurs, the plaster must be removed immediately, and a healthcare provider should be consulted. These precautions are taken seriously by practitioners, who conduct a thorough pre‑treatment assessment to screen for contraindications and to tailor the acupoint selection to the individual’s specific pattern of disharmony.
In recent decades, the dog‑day patch has undergone a remarkable transformation from a folk remedy into a standardised, evidence‑informed procedure offered by thousands of public hospitals and community health centres throughout China. It is now integrated into the national preventive health services, often covered by basic medical insurance for qualifying chronic conditions. This institutional recognition reflects a broader shift within Chinese healthcare toward preventive and integrative approaches, where traditional methods are systematically evaluated and refined through modern research protocols. Numerous randomised controlled trials have been published in peer‑reviewed journals, examining its effects on lung function, immunoglobulin levels, and quality‑of‑life scores in patients with asthma and rhinitis. A multi‑centre study involving over two thousand participants found that the three‑year course significantly reduced the annual exacerbation rate of chronic bronchitis by nearly forty percent, with the most pronounced benefits observed in middle‑aged and elderly patients who had suffered from cold‑induced cough for more than a decade.
Beyond its clinical applications, the summer patch therapy embodies a philosophical view of health that resonates with universal human concerns. It assumes that illness is not merely an acute event but a manifestation of underlying imbalances that can be anticipated and corrected in advance. By aligning treatment with the seasonal rhythm, it teaches a practical lesson in ecological medicine – that human physiology is inseparable from the external environment, and that timely, targeted intervention can forestall far more severe problems later. This forward‑looking, cyclic perspective offers a valuable contrast to the reactive, symptom‑focused model that often dominates acute care in Western medicine. For many patients, the annual ritual of visiting a clinic during the dog days becomes a meaningful health habit, reinforcing a sense of agency and continuity in managing their chronic conditions.
The therapy also demonstrates the enduring adaptability of traditional knowledge. Modern manufacturers have developed pre‑packaged, quality‑controlled plaster kits that reduce variability and improve safety, while clinicians have refined the dosing and duration based on pharmacokinetic data and skin‑reaction monitoring. At the same time, the core principles – the use of warming herbs, the selection of back acupoints, and the adherence to the summer calendar – have remained remarkably stable, indicating that the empirical wisdom accumulated over centuries retains its practical value even when subjected to rigorous scientific scrutiny. This coexistence of tradition and innovation is a hallmark of contemporary Chinese medicine, and the dog‑day patch stands as one of its most accessible and widely embraced expressions.
For international readers unfamiliar with this practice, it may initially seem exotic or even implausible. Yet a closer look reveals a coherent system of reasoning, supported by both historical experience and emerging clinical evidence. The treatment is not a miracle cure, nor is it a replacement for standard medical care; rather, it is a supplementary, well‑tolerated intervention that can improve symptom control, reduce reliance on rescue medications, and enhance overall resilience in carefully selected patients. As global interest in integrative and lifestyle‑based healthcare continues to grow, the dog‑day patch offers an instructive example of how a seasonal, acupoint‑based herbal therapy can be seamlessly integrated into a modern health‑management framework.
Ultimately, the success of this therapy depends on proper patient selection, precise acupoint placement, appropriate patch composition, and strict adherence to post‑application care. It is not a do‑it‑yourself remedy; every step should be supervised by a qualified practitioner who has diagnosed the patient’s constitutional type and confirmed the absence of contraindications. When these conditions are met, the dog‑day patch provides a safe, cost‑effective, and minimally invasive means of strengthening the body’s defences against the cold and damp of winter. In an age when preventive medicine is increasingly valued over reactive treatment, this ancient summer practice stands as a timeless testament to the wisdom of treating the root before the branch, and of using nature’s own rhythm as an ally in the pursuit of lasting health. For millions of people each year, those sticky little plasters on their backs are not a nuisance but a promise – a promise that the heat of July will help them breathe more easily in the frost of January.

